
CRP is an acute phase inflammatory protein that is elevated in both viral and bacterial infections. Bacterial infection is a potent stimulus of marked CRP elevation. Normal CRP is less than 3 mg/L.3 It has been demonstrated that 38-56% of patients with viral acute respiratory infections (ARI) have CRP levels greater than 20 mg/L which may lead to unnecessary antibiotics being prescribed.1 CRP levels may increase over 100 mg/L with adenovirus, influenza, and COVID-19 infections.4-5
MxA is an intracellular blood protein that is stimulated by interferon (IFN) alpha/beta.6 Interferons are induced by viruses and form an essential part of the immune system’s defense against viral infections. MxA protein becomes elevated only in the presence of acute viral infections and not in bacterial infections, making it an ideal biomarker for acute viral infections.7
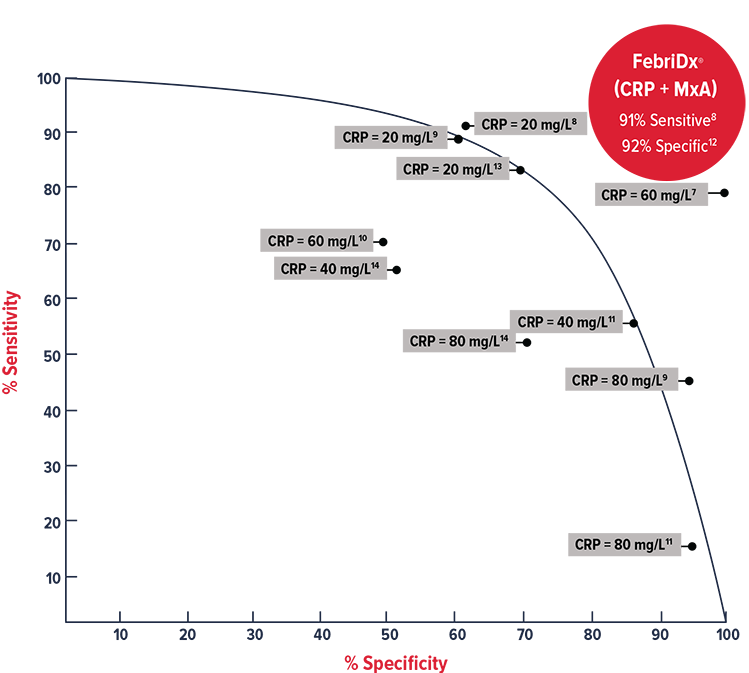
On their own, neither CRP nor MxA is sensitive or specific enough to differentiate viral from bacterial infections.7-14 At low levels, 20 mg/L, CRP is very sensitive, but non-specific, at confirming bacterial infection.8,9,13 At high levels, 80-100 mg/L, the reverse is true.9,11,14
MxA is specific for viral infections and will not be elevated in the presence of a bacterial infection.
By combining the acute phase inflammatory protein, CRP, with a specific viral marker, MxA, FebriDx® achieves high sensitivity and high specificity to accurately and reliably differentiate between viral and bacterial acute respiratory infections.
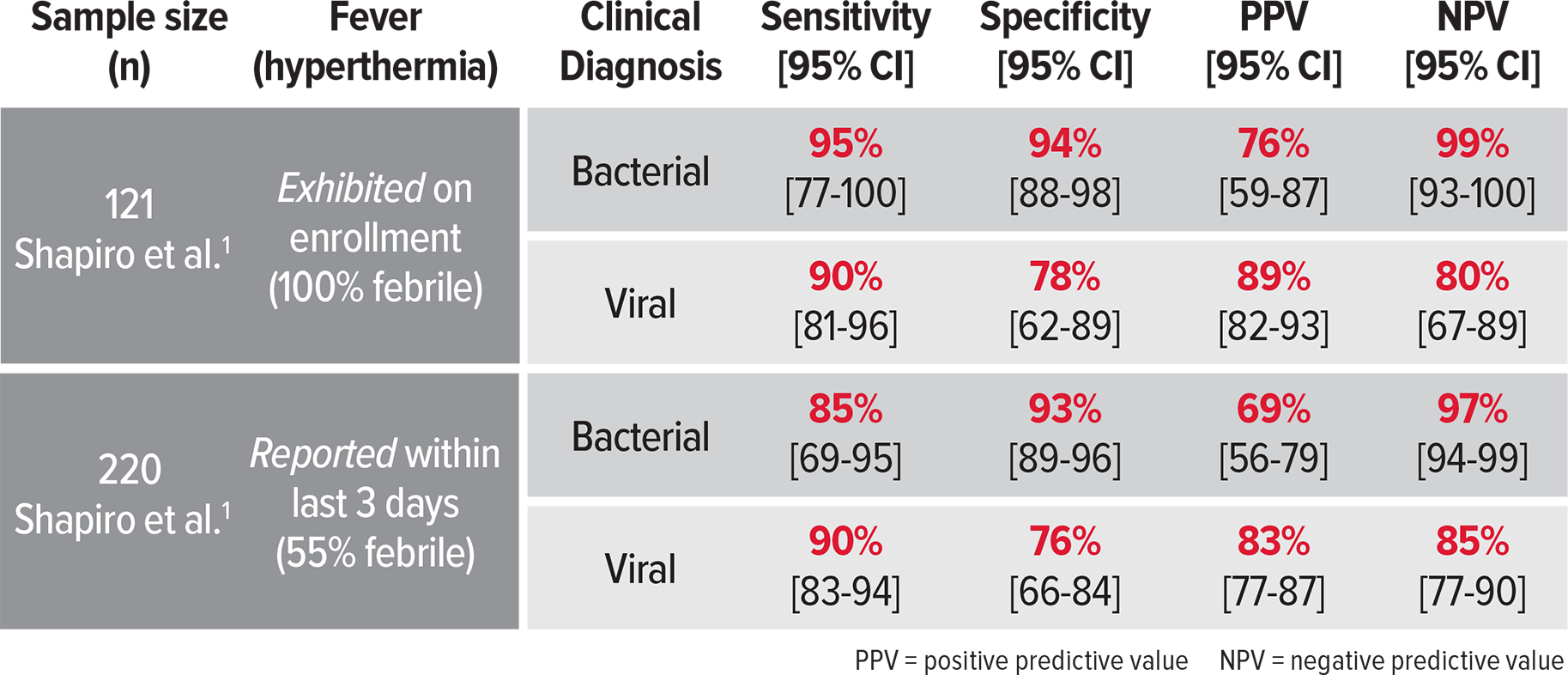
Multi-center prospective clinical trials demonstrated high sensitivity and specificity of FebriDx® in differentiating viral from bacterial acute respiratory infection.
Studies conclude a greater accuracy for differentiating viral and bacterial infections than CRP or procalcitonin alone. FebriDx® has a 97-99% NPV to assist in ruling out a bacterial infection.1-2
Acute respiratory infections are diagnosed and managed in GP settings solely by clinical signs and symptoms. Because viral and bacterial infections have similar symptoms, determining diagnosis and treatment by clinical observation alone may lead to misdiagnosis and unnecessary antibiotic treatment.
A FebriDx® test was performed on 21 patients (aged 3 years to 84 years) who had clinical diagnoses of an acute respiratory infection. In each case, a clinical diagnosis was initially made by a GP.
FebriDx® improved the clinical management in 48% (10/21) of the patients, including two patients that were clinically presumed viral but FebriDx® determined a bacterial infection. One of these patients was admitted to the hospital with sepsis.
FebriDx® safely reduced unnecessary antibiotics in 80% (8/10) of clinical cases without any adverse events. FebriDx® was concluded to have high sensitivity and specificity for identifying and differentiating viral from bacterial acute respiratory infection.15
